Fig. 1
Chapter 2
HOW MYOPIA DEVELOPS
Lengthening of the eye. Prevention requires a knowledge of causes. We need to understand what causes myopia to develop in the first place and what makes it continue to get worse. There is no doubt that as an eye becomes more and more myopic, it is becoming longer and longer. This has been determined by taking X-ray pictures of the eye, by using ultrasonic measuring techniques, and by other methods.
Fig. 1
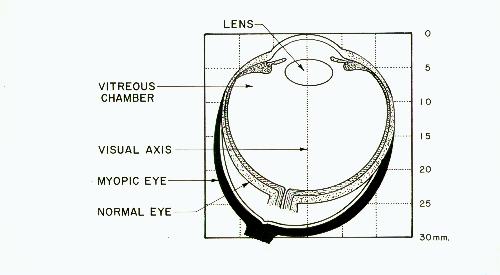
Figure 1 shows an eye that is highly myopic. Note how much the eye has been stretched from the round shape of a normal eye. Although not shown here, the coats of the eye become thinner as they stretch. This type of myopia is called axial-length myopia because it clearly results from an abnormal increase in the length of the eye along its visual axis. It is associated with a prolonged increase of pressure in the vitreous chamber inside the eye. The eyes of most myopes don't lengthen anywhere near this amount, of course, since only a small change from the normal in the axial dimension of the eye is sufficient to cause blurring of vision. Note that the part of the eye in front of the lens does not change.
Myopia occurs in two stages. The first stage is called spastic myopia and is reversible. That is, it can be eliminated by removing the cause. The second stage is the axial-length myopia mentioned above. It is irreversible. Spastic myopia involves the lens and it precedes the development of axial-length myopia. The permanent stretching of the coats of the eye only occurs if the spastic myopia is permitted to exist for too long.
Now we come to the heart of the problem - how too much close work causes myopia to develop.
Our eyes have evolved over many thousands of years and have thus become admirably adapted to the world we live in, However, we no longer use our eyes in the same way they were used during these many years of evolution. We no longer use our eyes as nature intended. Most animals on earth use their eyes mainly for distance. Only for brief periods do they look at close objects. Humans living in primitive, illiterate societies also use their eyes in much the same manner. It is in our modern, literate societies that this situation has changed drastically. With the invention of printing, the publishing of books, compulsory education, computers, and office work have come unprecedented demands on our eyes for prolonged close work. Our eyes were never designed for this type of use. They were never intended to be used for reading. Remember that normal eyes are at rest when looking into the distance. Looking at something close requires a strong focusing effort by the ciliary muscle which controls the shape of the lens of the eye. This puts the ciliary muscle under a more or less constant state of stress.
We all know what happens to the body of a weight lifter. By steadily increasing the weights used for training, the various muscles are repeatedly subjected to a condition of high stress. The muscles respond by getting bigger and stronger so that the work can then be done with less effort.
Something similar happens inside the eye. The ciliary muscle doesn't get bigger or stronger - it develops a temporary spasm. If a lot of close work is done, this spasm may exist for months or years. For this reason, I use the expression chronic ciliary muscle spasm to distinguish it from the acute ciliary muscle spasm that may develop for various other reasons.
It is this chronic spasm that initiates a process whereby the eye actually becomes larger. As it becomes larger it becomes more myopic and can do the close work with less stress. The eye thus has a very good reason for getting longer - so it doesn't have to work as hard! In both the myope and the weight lifter, the body is adapting so that a condition of excessive stress can be handled with a reasonable amount of effort. The unfortunate part of this process is that after the eye increases too much in length, it can no longer see clearly in the distance.
A ciliary muscle spasm does not develop in a few minutes or an hour and it cannot be eliminated in a short period of time. Accommodation must be maintained for long periods of time, day after day, before the spasm develops. To relax such a spasm, accommodation must be prevented or kept to a minimum for several weeks or longer. A ciliary spasm cannot be relaxed by a good night's sleep.
It is really essential only to understand that prolonged close work can cause the eye to get longer. It is not necessary for the average person to understand the mechanism by which the eye accomplishes this feat. But, for the sake of completeness, however, I am including here an explanation of what seems to be the actual mechanism of eye elongation:
PROLONGED CLOSE WORK
requires
CONSTANT FOCUSING ON NEAR OBJECTS
which causes
CHRONIC SPASM OF THE CILIARY MUSCLE
which causes
IRREVERSIBLE STRETCHING OF THE COATS OF
THE EYE WHICH SURROUND THE VITREOUS CHAMBER
(over a period of time)
which causes
INCREASE IN SIZE OF VITREOUS CHAMBER
resulting in
A MORE MYOPIC EYE.
Figure 2 shows the parts of the eye essential for this explanation. This is a normal eye making the necessary effort to focus a close object on the retina. This figure can be assumed to be an eye that has been cut vertically in half.
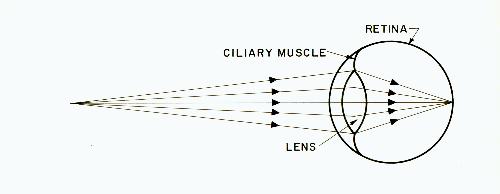
Fig. 2
When viewed from the side, as in figure 2, the lens is seen to be thicker in the center than at the edge. It is this curved shape that enables the lens to bend light rays. The thicker the center is with respect to the edges (called the periphery), the more power the lens has and the more it will bend the rays passing through it. To focus close objects, the lens must be made thicker than is needed for focusing distant objects.
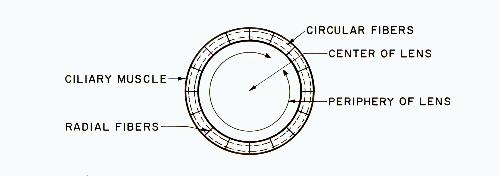
Fig. 3
Figure 3 shows the lens viewed from the front. The shape of the lens is controlled by the ciliary muscle, which is located behind the iris. The ciliary muscle surrounds the lens in much the same way that a ring surrounds your finger. If your ring suddenly became smaller it would tighten around your finger. The ciliary muscle, when its circular fibers contract, tightens around the lens in a similar manner. The radial fibers are thought to aid in relaxing the muscle.
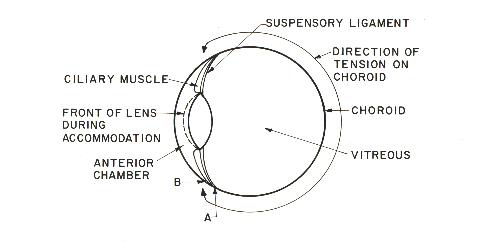
Fig. 4
Referring to figure 4, note that the ciliary muscle passes through the suspensory ligament and attaches to the choroid, and that the choroid extends all the way around the vitreous chamber. The retina covers the inner surface of the choroid. When the ciliary muscle tightens around the lens, it causes the lens to bulge forward as indicated by the dotted line. This makes the lens more powerful and enables it to bend the light rays more.
Increase in intraocular pressure. While the ciliary muscle is tightening around the lens, it is also putting tension on the choroid. Point A, where the ciliary muscle attaches to the choroid, is pulled forward to point B during accommodation. This tightening of the choroid around the vitreous chamber does not compress the vitreous fluid into a smaller volume (since liquids cannot be compressed as gases can), but it does cause an increase in the pressure in the vitreous chamber. When the pressure inside the eye (called intraocular pressure, or IOP) is measured by conventional methods, instruments are used on the surface of the cornea that actually measure only the pressure in the anterior chamber. This is the method used to test for glaucoma. The pressure in the vitreous chamber can be much higher. Tests on monkeys showed an increase in vitreous pressure of up to 6 mm Hg (six millimeters of mercury) during maximum accommodation.
Since the normal IOP in these monkeys is on the order of 12 mm Hg, it can be seen that the pressure in the vitreous chamber can increase by fifty percent just by focusing on a close object. The pressure in the anterior chamber, conversely, does not increase during accommodation but actually decreases somewhat. The anterior chamber and the vitreous chamber should be thought of as two entirely separate chambers.
During accommodation, the front of the vitreous body provides support for the rear of the lens as the ciliary muscle and choroid tighten. This tends to make the center of the lens bulge forward slightly into the anterior chamber and assists the ciliary muscle in making the lens thicker.1
Try to visualize that it is the ciliary muscle pulling on the choroid that causes the eye to stretch. The rise in pressure is merely an indication of this pulling, not its cause. It is for this reason that squinting does not cause stretching of the eye, even though it can cause the pressure inside the eye to increase temporarily.
As the coats of the eye stretch over a period of time, additional fluid moves into the vitreous chamber to fill the increased volume. This fluid can come from the anterior chamber where aqueous fluid is continually being produced and from where it can also escape to the outside. It is for this reason that in high myopia the vitreous becomes more watery than normal.
If this great enlargement of the vitreous chamber in high myopia was due to heredity, one would expect to find the vitreous chamber filled almost entirely with the normal jelly-like vitreous material. The fact that we find a watery substance, in addition to the normal vitreous material, should make it obvious that this enlargement is not due to heredity, but that it is abnormal and due to some harmful influence on the eye.
A momentary increase in vitreous pressure does not mean that the eye will elongate. It is only after a ciliary spasm has developed and causes a chronic elevation of vitreous pressure that elongation occurs. The eye that does not develop this ciliary muscle spasm does not experience such overelongation.2
It is important to remember that there is no known way to "shrink" the coats of the eye after they have been stretched. The situation is reminiscent of people in primitive societies who put weights in various parts of their bodies such as their ear lobes. Once these parts have been stretched, they will not return to normal even if the weights are removed. Because of this irreversible nature of axial-length myopia, prevention becomes exceedingly important. The eye moves in only one direction - toward increasing length. However, the first stage of myopia - spastic myopia - is reversible by relaxing the spasm, and the various techniques available to promote relaxation will be discussed in a later chapter. It is for this reason that children who have already become somewhat myopic can often be helped to regain normal vision rather quickly.
The normal eye. Lengthening of the eyes due to close work is normal. It is not due to "weak eyes" or anything of the sort. In fact, the mechanism described above is meant to play an important role in the development of everyone's vision. The normal child is born farsighted for a very good reason3- to provide a means of adjusting the eye to attain perfect vision as the child grows. The growth of the eye that follows birth can be divided into two parts. During the first three years, the growth of the eye is quite rapid and it attains near-adult size. This is called the infantile period and it leaves the eye still somewhat farsighted.
This is followed by much slower growth from age three to thirteen, called the juvenile or definitive period. During this period of slow growth, the "cushion" of farsightedness in the eye is used for the final refinements in the vision.
In order to see clearly, the farsighted eye of the child must accommodate even when used for distance. A ciliary spasm is meant to occur and reduce the farsightedness to near zero so that no (or very little) accommodation is needed for distance vision and the full amplitude of accommodation is available for close work. When this point is reached, the ciliary spasm is meant to relax of its own accord and halt the elongation of the eye. It is only when this process continues too far (because of an abnormal amount of close work), that the eye passes through the zero point into a myopic condition. The usual glasses that most myopic people wear actually make this process occur faster and go further than it otherwise would.
The eye is meant to attain its final size long before the body reaches its final height. In primitive societies where children are destined to do no significant amount of close work, the eye probably reaches nearly its final size not long after the age of three. The only reason that the eyes of many children move into myopia and continue to get longer into the teens and twenties is that they do an abnormal amount of close work.
As a general rule then, a certain amount of farsightedness in the young child is normal and plays an important role in making the eye elongate during growth. Only when the elongation threatens to go too far and create myopia do preventive measures need to be undertaken. One other aspect of this situation concerns the young child who is very farsighted. For one reason or another, a doctor might feel that such farsightedness should be "corrected" with glasses so that the child no longer has to accommodate for distance vision. A full correction of this type would be a mistake since this would eliminate an important factor in the growth of the eye and the eye would remain farsighted. On the other hand, an extremely farsighted child whose eyes do not move toward emmetropia must be considered as having vision which is not developing properly.
From this explanation of accommodation, it should be obvious that a small amount of farsightedness can be compensated for (by accommodation) and does not result in unclear vision. Myopia of any degree, on the other hand, cannot be compensated for and does result in unclear vision. A small amount of farsightedness is normal and is not cause for concern. Myopia is serious and is cause for great concern.